

Price Transparency is Already Working to Fix Health Care
Just not the way most people think. And without breaking the internet.

Remember how my last post somewhat brashly asserted that the Trump price transparency policy — taking on secret prices in health care — was already working better than expected?
I know what some of you were thinking — especially those of you who work in the health care space.
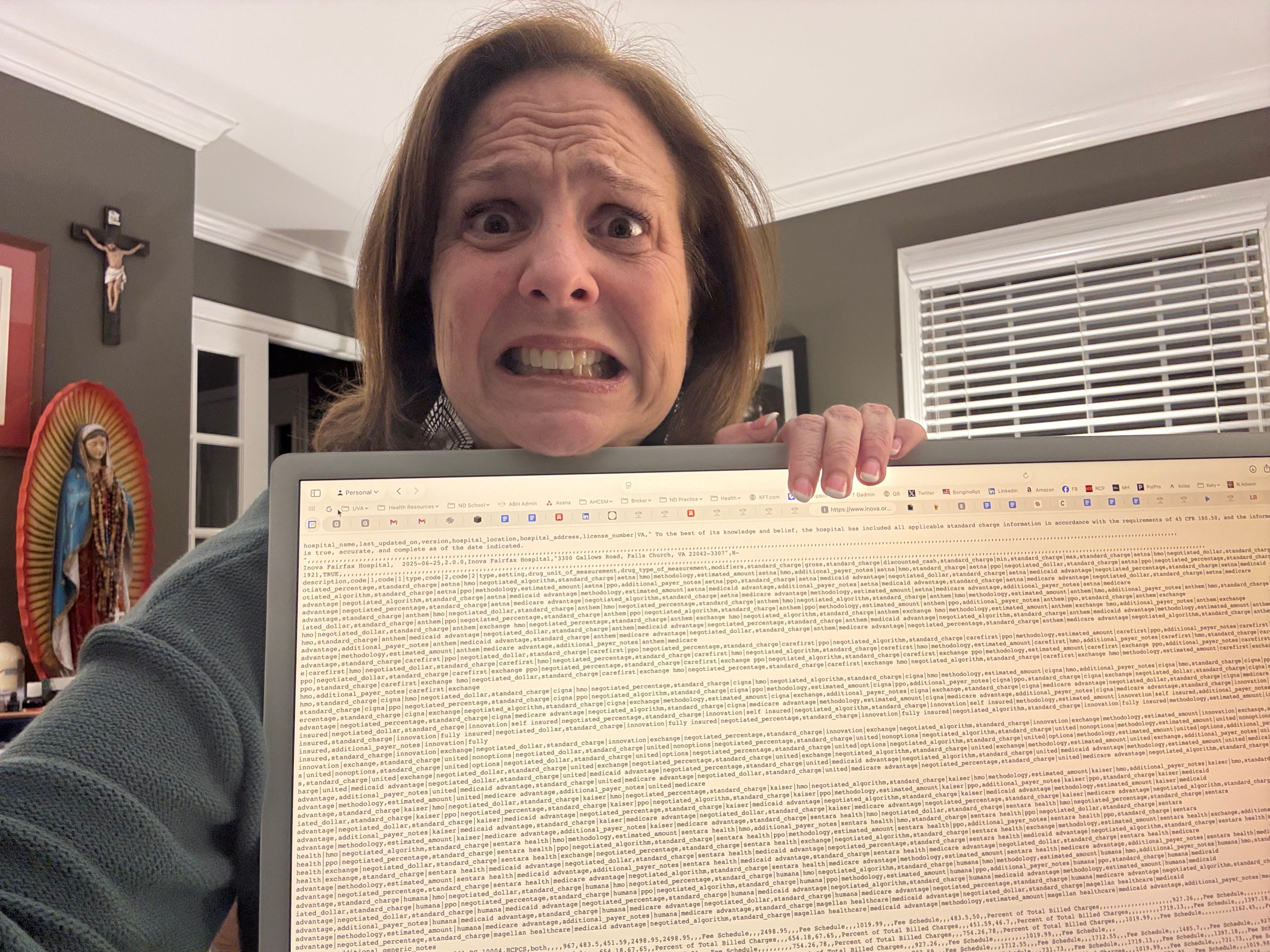
“Has she even SEEN those stupid machine-readable files the hospitals and carriers post? They’re unusable garbage! Price transparency is a joke!”
Fair enough! That’s certainly what everyone said would happen back in the day when we were fighting with industry, academics, and yes, my naysaying colleagues in the first Trump administration.
Why Hospitals Said Price Transparency Would Crash Their Websites (LOL)
The hospitals, like many others, argued that price information was all SO darned complex that:
It would be impossible to decipher even if it were public,
If deciphered, it would be impossible to use, and
If decipherable and usable, patients trapped in garbage insurance plans wouldn’t have the incentives to “shop” on price.
The hospitals caterwauled that they had so many different prices that the amount of data would literally crash their websites.
Because… insurers. Or something.
My initial response was:
“NOBODY IS HOLDING A GUN TO YOUR HEADS, making you charge 5 to 10 insurers 827 different prices for a Band-Aid.”
Yes, pricing is complex, conveniently so. The incumbent actors (hospitals, insurers, and drug makers) weaponize pricing complexity against purchasers because it serves their bottom line to do so.
I argued that price transparency would one day expose this weapon for what it is and demand would begin to arise for the Holy Grail so many of us have been chasing in health policy: pricing SIMPLICITY.
The Real Audience Wasn’t Patients
The demand for pricing simplicity — a single, knowable-in-advance price for something, no matter who’s paying — wouldn’t come from patients shopping.
Patients are trapped in their aforementioned garbage insurance plans, which aren’t set up to reward price sensitivity.
The truth is: patients were never the real audience for transparent prices — at least not at first.
Pricing simplicity is a big and important goal, but it’s not sufficient. Markets need consumers who have the ability to pursue lower cost and higher quality.
You can have price simplicity, of course, in some situations.
Like Dr. Keith Smith’s Surgery Center of Oklahoma, where there’s one low, all-in cash price for each procedure, no matter who’s paying.
That’s pricing simplicity, par excellence.
But the problem is that the only consumers interested right now in that simple price is an individual consumer in the cash economy:
Someone who has a health savings account and an exceptionally high deductible (higher than the cost of a surgery),
A member of a health care sharing ministry that requires self-pay upfront before receiving financial support from the community afterwards, or
A mogul, who can afford to pay cash for everything and risk being uninsured.
Apart from a small group of innovative employers (like my clients, just sayin’) working with physician-owned surgery centers, Dr. Smith’s solution isn’t scalable to all health care providers everywhere (yet), because most patients don’t fall in those categories.
Three Podcasts, Three Reasons To Smile
And that’s why I smiled at a few recent episodes of my favorite podcasts.
On the first one, An Arm and a Leg, host Dan Weissmann’s guest, the incomparable Dr. Vivian Ho of Rice University, laid out her research about how price transparency has exposed something — we have no way of knowing whether the prices posted are what are actually being charged.

In other words, the vendors, startups and employers who are trying to make use of the complex pricing data might not be getting the most actionable information to drive financial performance.
So what’s so great about that news? Two things:
People are starting to try to use the price information to do important things. And they’re having trouble because the data aren’t good enough.
It’s getting them mad. The hide-the-ball reindeer games that hospitals and insurers play — while pretending to comply with price transparency rules — are exposing just how much these special interests must have to hide.
Price transparency rules, even when badly complied with, are generating demand for price information, and anger when it’s not available.
Mission number one of price transparency, check!
The second podcast that made me smile was Relentless Health Value, where host Stacey Richter’s guests Dr. Sam Flanders and Shane Cerone laid out the problem: they took over a hospital and decided to make it great again. They brought the quality scores up from the basement to A+, and they restructured pricing to be more than 50 percent lower than what most hospitals charge. And then they waited for the stampede of patients, employers, insurers and other purchasers of care to come.
And they waited some more.

Weird, right?
I mean, markets reward lower prices and higher quality. I was reliably informed by all my free-marketeer colleagues inside the Trump administration that The Market™ was so amazing that it must not be micromanaged with silly price transparency rules.
I argued back: “there is no market in health care.”
To repeat louder for the back of the room:
THERE IS NO MARKET IN HEALTH CARE.
Not only do we not have easily knowable-in-advance and accurate prices, but what the podcast guests described so well is that markets also require consumers who are both:
Interested in, and
Able to respond to price and quality.
What Dr. Flanders and Mr. Cerone explained is that insurers are able to respond but not interested (hurts their bottom line, counterintuitively).
And insured people might be interested, depending on the structure of their cost-sharing obligations, but they’re not (usually) able to respond collectively enough to lower prices at scale, since they don’t make the decisions about which providers to include in their plan’s network and what to pay them.
Uninsured rich people might be both interested and able to respond to price information, but there aren’t enough of them to move the needle.
Here’s some math for the STEM crowd:
No prices + no consumers (if there were prices) = no market.
Why This is Actually Good News (I Know, Weird)
So, again, why is this good news?
Because people have started to notice.
Not just wild-eyed Trump staffers in 2018 with theories about what a market is.

But lots of podcasters, hospital executives, health policy influencers and, most importantly, bulk purchasers such as employers, unions, governments and health care sharing ministries.
These are the only potential actors out there who are both interested in and able to respond to pricing information if they have it.
Until now, they haven’t been consumers of health care.
They’ve only been consumers of health insurance, quaintly assuming that health insurance was the way — the only way — to get lower cost health care.
And now, price transparency has exposed just how wrong they were — in the best way.
Health insurance is a scam and, thanks to price transparency rules, the industry’s main customers — bulk purchasers of insurance — know it.
The third podcast that made me grin ear-to-ear was another Relentless Health Value episode featuring Elizabeth Mitchell. Elizabeth is helping jumbo employers — the bulkiest of bulk purchasers — use price transparency data combined with safety and quality data to shame their brokers and carriers, hopefully resulting in both being fired en masse.
They’ve realized they’ve been lied to. For decades.
The Holier Grail: When Bulk Purchasers Finally See the Scam
And that, my financially exploited friends, is the Holier Grail: getting bulk purchasers out of the market for health insurance because they can finally see how it fails them:
They pay more with insurance than without it (i.e. cash).
The network price at one hospital is often multiples more expensive than at the hospital down the street, for no discernible reason. Worse, employers’ contracts with their insurer bans them from doing anything about it (like steering patients away with plan design or negotiating their own, better contract with that hospital).
Network prices are usually all equally bad, net-net. Blue Cross is better at one hospital, United is better at the one down the street. But the variation is not systematic and it’s all a wash in the end, almost as if these networks were colluding to ensure that there was no meaningful price competition.
Once bulk purchasers see all this, their next thought is, well, despair.
The prices are set by secret contracts between hospitals and insurers that they’re not party to, but which bind them and their workers, who bear the dire financial and medical consequences.
They recognize that insurers are just using them as dupes in a corrupt scheme to profiteer and prey upon the sickness of the American people and the asymmetry of knowledge between the sellers of insurance and the buyers of insurance.
When they finally see all this, they get mad enough to try some crazy ideas.
A subsequent article will outline what some of those crazy ideas should be (an even HOLIER Grail and eventually the Holiest Grail of all) and what it would take to really get there.
Price transparency was never intended to be the wholesale solution to a missing health care market.
It may not be the end of insurance and its fraudulent promise to get health care to people at lower cost, but it’s a long overdue beginning of the end.
P.S. After you subscribe, come find me in the comments. I want to hear your price transparency horror stories. Or victory laps. Both are welcome here.
And here are the links to the excellent podcast episodes referenced above:
An Arm and a Leg- DanWeissmann and guest Dr. Vivian Ho of Rice University.
Relentless Health Value - Stacey Richter and guests Dr. Sam Flanders & Shane Cerone.
Relentless Health Value Stacey Richter and guest Elizabeth Mitchell.
Our company insurance is outrageous and even though they pay a good bit me and my employees continue to get bills after care from hospitals with increasingly higher prices. What is the best option for us or what should I look into to help my employees lower costs? Because right now they and Myself spend a fortune on medical bills on top of the already outrageously high insurance premiums that include super high deductibles.
Great commentary, Katy. You mix experience, common sense and humor. I have visited the Surgery Center of Oklahoma with my colleagues from AAPS. Of course CON makes it impossible to clone his surgery center in many other states.