

The Science We Skipped
Warning: interrogating virology’s founding myths may cause headache and disorientation


Editor’s note: This is Part 1 of a two-part series interrogating the foundational evidence behind modern virology. Part 1 covers how viruses are reportedly isolated. Part 2 covers genome sequencing, PCR testing, and viral antibody science, built on the same foundation.
I was a second class citizen in my public health school’s department of Epidemiology.
Harvard was ground zero for chronic illness research, best known for the Framingham Heart Study and the Nurses Health Study. All the cool kids were on the chronic disease epidemiology track. I wanted to study infectious disease instead. That’s why Johns Hopkins had actually been my first choice. I had signed the papers, submitted the deposit, and found an apartment in Baltimore a few months before the semester started.
But then, a funny thing happened.
I got a notice that Harvard was offering me a full ride - free tuition. Stick with me, this isn’t the humble brag it sounds like. One does not turn down free degrees from the Kremlin on the Charles, boring chronic disease specialty or not. So I got out of my lease in Baltimore, and re-directed to Boston.
A week after I got there, the financial aid office told me there’d been a mistake. A doctoral student with my same last name was the intended recipient of the money. They were bound to keep their word for my first year, but the rest of my degree would be paid by student loan (i.e. me).
God has a funny sense of humor.
Clearly, it was meant to be. It’s where I met former FDA Commissioner, Marty Makary, as I wrote about a couple weeks ago. It’s where I met the tropical health professor who recommended me for a job in South Sudan, where I realized overseas work wasn’t for me.
I had discovered epidemiology (which, before COVID, most people couldn’t pronounce, much less define) because I hated lab work.
I was pre-med in undergrad, loved studying human biology, but detested the pipettes and petri dishes in lab work. I preferred the methods of social science - statistics, graphs, p-values and regressions. It wasn’t until I was reading The Hot Zone, by Richard Preston, which was published the year I graduated from college, about an Ebola outbreak in a lab facility in Reston, VA (practically my hometown), that I ever heard the word “epidemiology.” Turns out, it combines the content of medicine with the methods of social science - a great fit. Individual patients, phooey - we treat populations!
Maybe it’s because my first introduction to public health and epidemiology was with Ebola in the Preston book, but infectious disease always seemed WAY sexier than chronic disease. Chronic disease involves the tedious and disappointing slog of changing people’s lifestyles and long-held habits, yuck!
Infectious disease - now that’s an adventure.
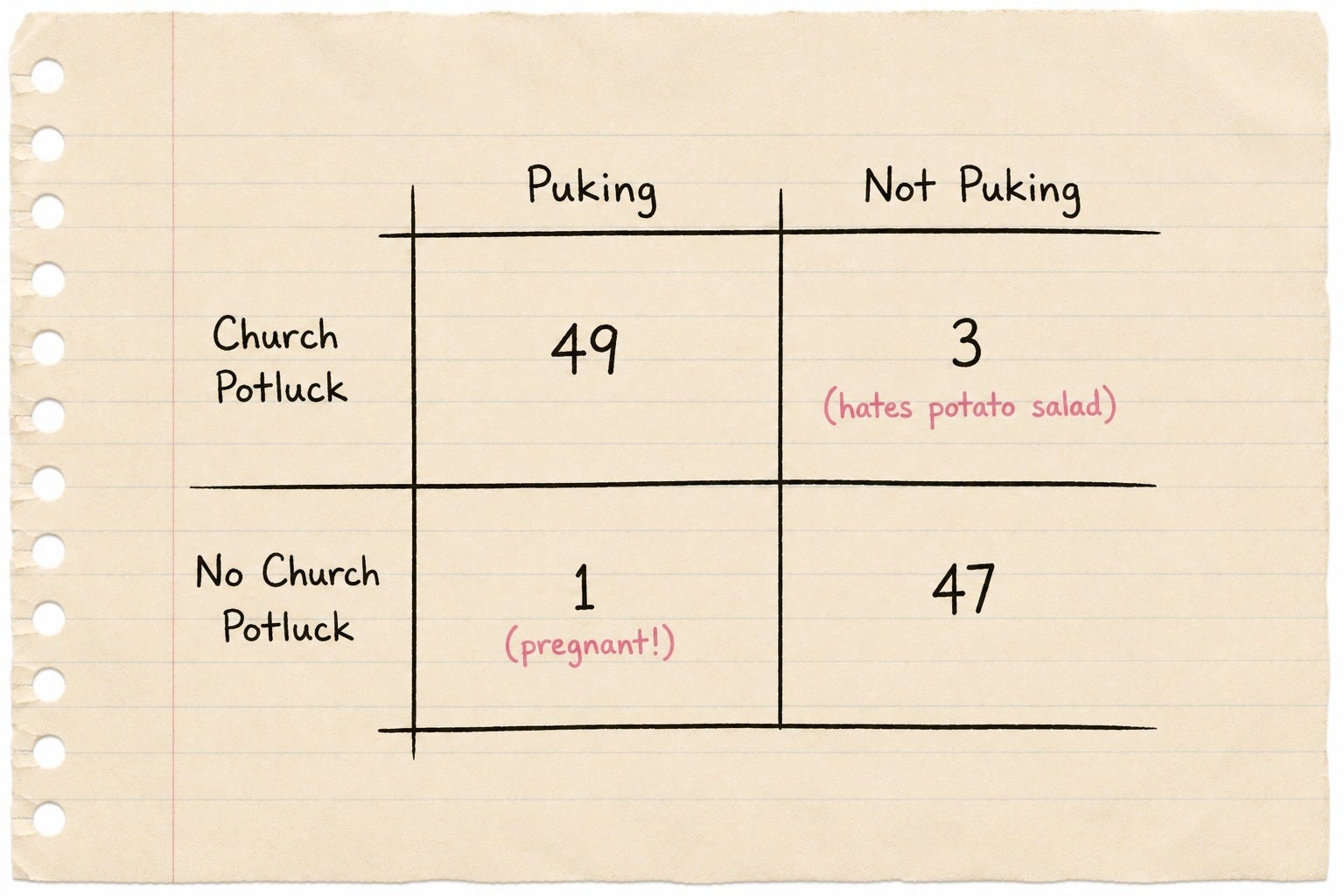
You get to run around in space suits, tell everybody what to do, quarantine towns, and use little hand-written tic-tac-toe crosstab charts to figure out what caused the outbreak (PS it’s always the potato salad at the church supper, at least in all the case studies).
And like legendary Dr. John Snow (no, not the Game of Thrones hottie) did when he shut down the contaminated London well responsible for spreading cholera, we infectious disease epidemiologists always had some magical intervention that would save a zillion lives and our names would live in glory evermore.
Unlike the Harvard chronic illness people, who kept getting things wrong when it came to the causes of heart disease, whether saturated fat was bad or good, and who failed year after year to get people to change their diets, exercise more, and quit smoking, while the population got sicker, fatter, more infertile and more expensive with our extinction-level chronic illness rates, infectious disease epidemiologists were able to actually, you know, end diseases, and save people. Fast. That was my take, anyway.
Now, even among the infectious disease crowd, there were the cool kids and the not-so-cool kids.
The real weirdos were the experts in rickettsial diseases or chlamydia. Then you had the middling workhorses, serious scientists focused on things that killed a gazillion people every year - respiratory disease, tuberculosis, diarrhea, malaria. But the coolest kids in school were the virus hunters. So, naturally, that’s what I wanted to be - hunting down strange new concoctions like hantavirus, Lassa fever, dengue hemorrhagic fever, you get the point. If it involves bleeding out of the eyes, I was all in.
The most pathetic virologists were those, like Dr. Fauci, who studied viruses that supposedly caused cancer or other chronic illness. I mean, the whole point of being a virus hunter was to avoid the complicated humanity of chronic illness - what a career face-plant!
Not sure if I was an adrenaline junkie or what (my later career in politics suggests as much), but I was high on the idea of being on a CDC rapid response team jetting around the globe to save people with the power of my mind or some other Dr. Snow-ish intervention.
An example was when I interned with the Carter Center on their guinea worm eradication program in South Sudan. Guinea worm is a parasite that grows into a multi-foot-long worm that slowly emerges, a little bit more each day, from the body over weeks. There is no treatment except to wrap the part of the worm that has already emerged around a little stick and then twist the stick every day a little more to try to expedite the emergence. Sometimes it comes out of nipples. Sometimes out of eyes. Usually though, less exotically, out of feet.

It burns like hell, and so people would run to the nearest water source and put their foot in the water, releasing all the parasite babies into the water, which people drink back into their system and the cycle continues. So the brilliant, Dr. Snow-ish intervention? Put a cloth filter over everyone’s water jug. Filters out the parasite babies, problem solved, disease eliminated from everywhere it was successfully implemented community-wide.
Do you see the appeal? It’s all so simple.
When we had the 101 classes in the infectious disease track, we studied the different bugs - bacteria, parasites, viruses. In the virus section, we learned what a virus was - a self-replicating piece of genetic code (DNA or RNA) and some proteins thrown in for good measure, which can enter through a cell membrane, hijack the gene-replication apparatus of the cell, replicate itself, bust open the cell membrane and travel to other cells and do the same thing. Viruses can be transmitted by bodily fluids, on objects like door handles, or in the air. There are no really great antiviral treatments that directly kill viruses the way antibiotics kill bacteria, so prevention is the best strategy. That’s it, that’s the 101. Or at least, that’s what I was taught.
You might be surprised to learn what we did NOT learn.
Namely: how these viruses were discovered, isolated, observed, cultured, and experimented upon. In other words, everything that we were taught about what viruses are and what they do was taught as a given. It wasn’t explained how The ScienceTM had proven all these facts. That should have been in the 101, but it wasn’t.
I only figured that out later. A lot later. Like a few years ago later. After an entire career built around on-the-ground programs, and later, policy design and program oversight of government agencies in charge of controlling viruses such as hepatitis, HIV/AIDS, HPV, and yes, coronaviruses.
This article series is my attempt to shorten that cycle for you, so you don’t fall into the traps I did.
(Many of you already know this, even better than I do, and I’m grateful for the groundbreaking work and courage of those who have been bringing this information to light.)
This is going to be the 101 I wish someone had given me back in public health school. Because it probably would have changed a lot about what I did next.
So where did we come up with this whole virus idea in the first place?
Bacteria and parasites are living/swimming organisms that we can see under basic light microscopes. So they were understood better at the beginning of the 20th century. The problem for The ScienceTM at that time was that there were some illnesses where they couldn’t find any bacteria or parasites present. So they hypothesized there might be something else. Maybe a teeny tiny other thing that didn’t yet have a name. Maybe virus?
So they started taking sludge from sick samples (sap from sick plants, snot from sick people, etc) and pushing them through filters to try to filter out the bigger bacteria/parasites and see if what got through the filter still seemed to cause illness in previously healthy organisms. The problem? The mode of transmitting to healthy samples was pretty damaging in and of itself. There was mechanical injury in the transfer. Also, there weren’t always controls (healthy samples receiving the same toxic sludge EXCEPT the sick organism’s fluid), and when there were, often the controls would experience some or all of the same symptoms as the “infected” samples.
These experiments never disproved the virus theory outright (though some came close). But neither did they prove it. They only demonstrated that something was making the healthy samples sick after “inoculating” them with the sick organism’s fluid. But even that wasn’t entirely clear. The problem is that, in many experiments during the first half of the 20th century, including pivotal ones by John Enders, and Bech and von Magnus, the controls got sick too.
In the Spanish flu pandemic around 1917, researchers tried everything to make healthy volunteers sick by having sick people coughing on, shaking hands with, spraying lung gook in the faces of, transfusing the blood into, and injecting sputum into the volunteers - to no avail. Weirdly, mainstream virology and news reports often selectively leave these confusing facts out and students are never taught it.
In any case, something other than identifiable bacteria or parasites can make healthy organisms sick in some experiments, but the something isn’t always identified well. In the case of the virus experiments, it could be the toxic crap in the base exposure of both the “inoculated” and the controls, and not something specific to the sick organism. The facts on this vary by the details of each experiment, which we’ll discuss further below.
The early researchers acknowledged that they didn’t know what this smaller “agent” or “exposure” was, but they called it “virus,” the latin root of which simply means toxin or toxic fluid. Quite a big distance between that and the specific, self-replicating DNA/RNA+protein definition that we are taught today.

So How are Viruses Isolated?
Virology has not advanced much more than the seminal “isolation” experiments by John Enders and Bech and von Magnus in the 1950s.
Here are the steps that we still use today:
A sample is collected from a sick person - typically a nasal swab, blood, or throat washing. This material contains everything present in that person’s body at that site: dead cells, cellular debris, bacteria, fungi, exosomes, proteins, and whatever else is there. It is not purified or filtered at this stage.
Antimicrobials - typically penicillin, streptomycin, and often amphotericin B - are added to the sample in large doses to kill bacteria and fungi. These antibiotics and antifungals are themselves cytotoxic (especially to kidney cells), meaning they are toxic to cells at the concentrations used.
The sample is now added to a cell culture - usually a line of monkey kidney cells (Vero cells are the current standard, derived from African green monkey kidneys), grown in an artificial nutrient medium. These cells are already stressed by definition: they have been removed from their natural environment, grown on plastic, fed an artificial mixture of nutrients, and kept alive under conditions nothing like those inside a living body.

The nutrient medium (the food for the cells) is fetal bovine serum (FBS) or in layman’s terms - fetal cow blood. FBS is harvested by stabbing a live cow fetus in the heart with a large-bore needle, after the mother is slaughtered (you can imagine the stress/cortisol/hormone profile of the living fetus at that point). FBS is used because it contains a complex mixture of growth factors, hormones, and proteins that keep the cells alive in their artificial environment. Without it, the monkey kidney cells would automatically begin to die. FBS is not a defined, standardized substance - its composition varies batch to batch and contains unknown quantities of baby cow proteins, lipids, growth factors, and critically, cow genetic material and any contaminants in the blood of the baby cow.
At the same time that the sick sample (the snot, blood or other fluid from the sick person) is added to this cell culture being kept alive in a very artificial environment by fetal cow blood, the researchers simultaneously attempt to take away as much of the fetal cow blood as they can. This is because it’s thought that the FBS interferes with the virus’ ability to penetrate the monkey kidney cells. The problem is that the hour or two without food intensely stresses those cells, which were already on the verge of death. They begin to show signs of breaking apart and deterioration that is later attributed to the virus. So at that most important moment - when the supposedly virus-infected patient sample is introduced to the cells, they are already freaking out.
After about 1-2 hours of absolute starvation, a little bit of FBS is added back - but between 10-20% of the amount it was before it was initially withdrawn. So now the cells have just spent 1-2 hours in total starvation, and then they’re given enough food to merely be mostly starving.
When the cells show the predictable and inevitable signs of chaos and death, this is called cytopathic effect (CPE), and is attributed solely to the presence of the virus. I’m not kidding.
But just because the virus is presumed to be present in the sludge doesn’t mean that it’s been isolated, that is, separated or purified out of the sludge.
So then they take the sludge of dead and dying, poisoned (with antimicrobials), starved and environmentally stressed cells, and they throw it in a centrifuge. This separates out all the different ingredients in the sludge into layers of pellets based on size/density. But there can be tons of different things in the pellets containing similarly-sized particles.
Then they take a certain pellet - the one that is the size that the virologists already “know” is the size of the virus they’re trying to isolate (see how circular that is?) - and they throw it under an electron microscope (because a regular light microscope can’t see stuff as small as a virus is alleged to be).
When they identify some debris or other particle that seems to be present in some high quantity, they call it the virus. And the first guy to characterize some particular shape gets the right to name the virus and the disease that supposedly is caused by it in the patient from whom the snot, blood or whatever was taken. Then that shape becomes the “standard” way of identifying that virus later, so that when virologists are isolating viruses that they already “know” about, then they just look for the particles that match the shape that some researcher once called the virus. The squiggly snake is Ebola, the spiked ball is coronavirus (if the spikes are numerous), or influenza (fewer spikes), or HIV (same size but slightly fewer spikes) - get it? They’re TOTALLY different, for realz.
The tricky thing here of course is that the debris from dying cells, such as exosomes, as well as artifacts that are known to appear in electron microscope visualizations are also similar-looking.
So, you might be saying to yourself: “Self, I have questions about this process.”
Yeah, you wouldn’t be the only one.
In fact, a few years ago, the German virologist Stefan Lanka decided to call bullshit on this process, and he made a public promise to pay 100,000 Euros to anyone who could provide scientific evidence that measles is caused by a virus, specifically by publishing a single paper that:
Proved the existence of a measles virus
Showed its diameter
Showed its genetic information (more on that next week)
Showed that it caused measles.
A German physician named David Bardens submitted six papers collectively purporting to satisfy the criteria. Lanka wasn’t convinced and he didn’t pay. Bardens sued.
A lower court found for Dr. Bardens and ordered Lanka to pay up. But Lanka appealed. And at the appeal, the court commissioned expert testimony from an independent virologist who largely supported Lanka’s criticism of the “isolation” methodology. Lanka prevailed.
The court held there had been no definitive proof presented.
Mainstream reports didn’t correct their earlier headlines about Lanka having lost and been disgraced. Of course they didn’t.
Meanwhile, Lanka conducted his own experiments to replicate the Enders isolation procedure - but this time without any “viral” sample from a sick patient. He worked with a contract laboratory to perform the procedure described above exactly, but without the supposed virus present. His published paper reported the same finding as Bech and von Magnus - the same cytopathic effect occurred in the uninfected monkey kidney cells - which supports the idea that it’s the toxic sludge, starvation, stress and environment that is killing the cells, not a virus.
Final thoughts with that in mind.
I spent an entire career working to control epidemics caused by viruses, those tiny microbes I was never taught to question, and without a foundational understanding of how viruses are actually proven to exist: a centrifuged slurry of snot, monkey kidneys, antimicrobials, fetal cow blood, and a cell starvation protocol enshrined as gospel.
Followed by seventy years of The Science ™ stacked on top of this weird theory, with nobody asking what actually proves the foundation.
I’m not saying viruses don’t exist.
I’m saying I don’t know what we’ve isolated (if anything) - and neither does anyone who learned what I learned, the way I learned it, if they’re being honest about it. I’m embarrassed for my profession and every virologist who spends their days doing this sludge-technique over and over again and calling it “isolation.”
So that’s the viral isolation problem. But isolation is only the first of many questions.
Next week we go down the genome sequencing rabbit hole. Spoiler alert: it doesn’t get better.
Note to paid subscribers: there are many physicians, scientists and other experts whose work has schooled me on this subject in recent years. If you’d like a technical deep-dive to check my homework on this, I recommend the short book by Dr. Mark Bailey - just DM me and I’ll send you the public link to the free version of his book, Farewell to Virology.
Not surprising that assumptions have been made without following the science we pretend to worship. The world has is a long history of telling people what to believe without proof. And in most of those cases, people who ask questions are not celebrated.
HIV, herpes, HPV, SARS-Cov-2, the common cold . . . . The explanations for all of these are full of holes.
Thanks for this fantastic article, Katy. And thanks for allowing free subscribers to comment. 😁