

How to Lower U.S. Health Care Costs by Needing Less Health Care. Part 3: Hospital Edition.
Hospitals don’t provide health care. They’re where you go for financially abusive sick care after health care has failed.


Editor’s note: This is Part 3 of the series “How Do We Lower the Cost of Health Care in the U.S.? Need Less Health Care.” Part 1 changed the framework and how you think about healing. Part 2 covered what to do when something’s wrong, but not urgent, and the alternative pathways outside the conventional system. Part 3 covers what to do when you genuinely need a hospital, and how to choose one that won’t bankrupt you or make things worse.
I’ve already told you about my dying sister’s catastrophic night, strapped to a gurney and shipped across town at midnight because “there’s a bed open now.” I’ve told you about my daughter, three centimeters dilated and forced into an unbiological 12-hour deadline, because everyone’s on the birth assembly-line clock. Regular readers know I don’t romanticize hospitals. I’ve called them Soviet-style hellscapes, and I stand by it.
But this isn’t that article. This is the practical one.
Because despite everything we covered in Part 1 (get your mindset right, your body can do more than you think) and Part 2 (when something’s wrong, there’s a whole world of healers outside the white coat system), sometimes you actually need a knee replacement. Sometimes you get cancer and you want conventional chemo. Sometimes it’s a hernia repair.
When that day comes, you have a choice most people don’t realize they have: whether to hand yourself over to a greedy, bureaucratic, medically dangerous hospital system, or get the exact same care somewhere that won’t financially and clinically wreck you in the process.
The Tell
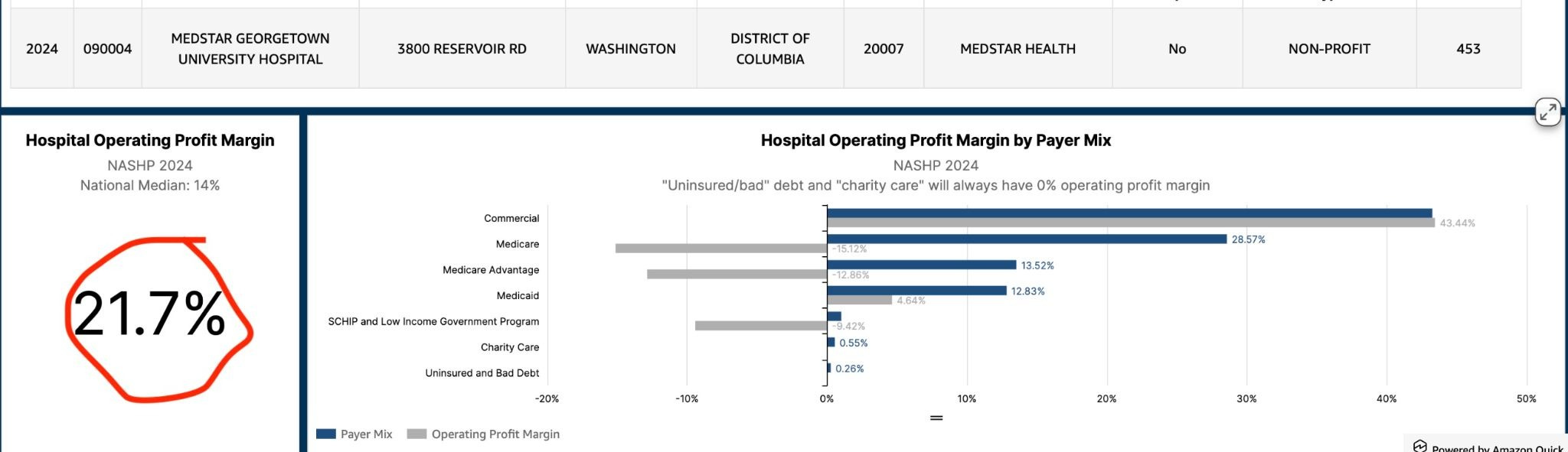
If you ever needed proof that hospitals are raping and pillaging their own communities, look no further than the hospital cost interactive tool, a delightful little playground built by the incomparable Marilyn Bartlett for the National Academy for State Health Policy (NASHP). The tool also feeds a wonderfully useful interface, Sage Transparency, that combines quality data with the NASHP cost data.
The tool pulls from every hospital’s actual, required financial filings to the government - because they wouldn’t lie to the government, right? Their real costs. Their liabilities and debts and private equity and hedge fund investments. Their charity care. Their mix of money-losing Medicaid patients, break-even Medicare patients, and commercially insured patients who are, in every sense of the phrase, the golden goose.
But the best part of the tool is the number it hands you called the commercial break-even rate - the percentage above Medicare rates a hospital would actually need to charge insured patients just to break even. No profit. Just breathing room.
Spoiler alert: that number is almost never higher than 50 percent above Medicare rates. So that’s what they’re charging, right? Because, they’re charities?
Not exactly.

Per the RAND Corporation’s ongoing hospital price transparency study, hospitals actually charge private insurers an average of 254 percent of the Medicare rate - outpatient services run even higher, at 279 percent. That’s a three-times markup over what it takes to survive, extracted from patients, employers and taxpayers.
But they’re dying, you see. DYING. They have to close their doors, dying! They have to send Grandma to collections, because, dying.
If these institutions were the white-hat charities their tax status pretends they are, they would charge no more than the commercial break-even rate to you and your plan. The fact that they routinely charge nearly double that or more tells you everything you need to know about who they actually are.
The Bait-and-Switch
At the end of the day, the “health care” system is dressed up as a haven of healing, when really it’s an altar of sacrifice demanding our dignity, our autonomy, our agency, and too often, our ability to get better. The medical system profits most when we are sick, sick for life, and have high-priced stuff done to us or bought for us. That’s the opposite of our own priorities, which are to be healthy, and to pay less. All the incentives in the system are aligned against those priorities.
We’ve discussed in this space before how hospitals are clinically dangerous hellscapes unfit for humans. But they are also deeply dangerous to our financial health. This is one of the main reasons Step Three of this whole series matters so much: stay the hell out of hospitals for non-emergencies.
Here’s the fuller rap sheet, in case you needed more convincing:
They wave their “nonprofit” status like a halo - billboards at the ballpark, Jesus-adjacent mission statements on the website - while hiring the priciest management consultants money can buy to make sure as few poor patients as possible ever find out about the free financial aid they’re legally required to offer.
They collude with insurers to force you and your employer to pay anticompetitive contracted prices instead of the (usually lower) cash price, and refuse to take cash from patients whose plans they’re contracted with.
They charge you a facility fee for the privilege of walking through their doors - a fee an identical, non-hospital-owned building down the street doesn’t charge for the identical service.
They’re rolling out AI in the exam room, marketed as freeing your doctor to look at you instead of a screen, when a good chunk of what it’s actually doing is mining the visit for more billing codes.
They’ve eaten nearly every independent practice and facility in sight, using monopolistic, cartel-like tactics to erase competition - which is exactly what that DOJ lawsuit against OhioHealth was about (which OhioHealth recently settled).
They exploit the 340B drug program (h/t Dutch Rojas) - a safety net program designed to help free clinics and HIV providers stretch scarce dollars for poor patients - by buying drugs at pennies on the dollar and then billing plans and patients full price, pocketing the spread.
They turn outpatient visits into revenue funnels, pressuring employed doctors to refer patients to pricier services inside the system, corroding the trust between doctor and patient and grinding down the souls of well-intentioned physicians in the process.
They charge you whether they heal you, cure you, or make you worse - and they cover up the errors and the inhumane staffing conditions that produced them.
They create the very complications they then bill you to treat.
They hide their prices behind contract gag clauses and simply ignore the federal transparency rules when the fines are cheaper than the exposure.
They prohibit self-funded employers from cutting a better direct deal with them than their insurer already negotiated.
They’ve even gamed Medicare’s rural and urban hospital designations (h/t Alex Berenson) simultaneously - claiming rural status for one payment program and urban for another - to squeeze extra money out of both. HHS tried to force hospitals to pick a lane. A federal court struck the rule down.
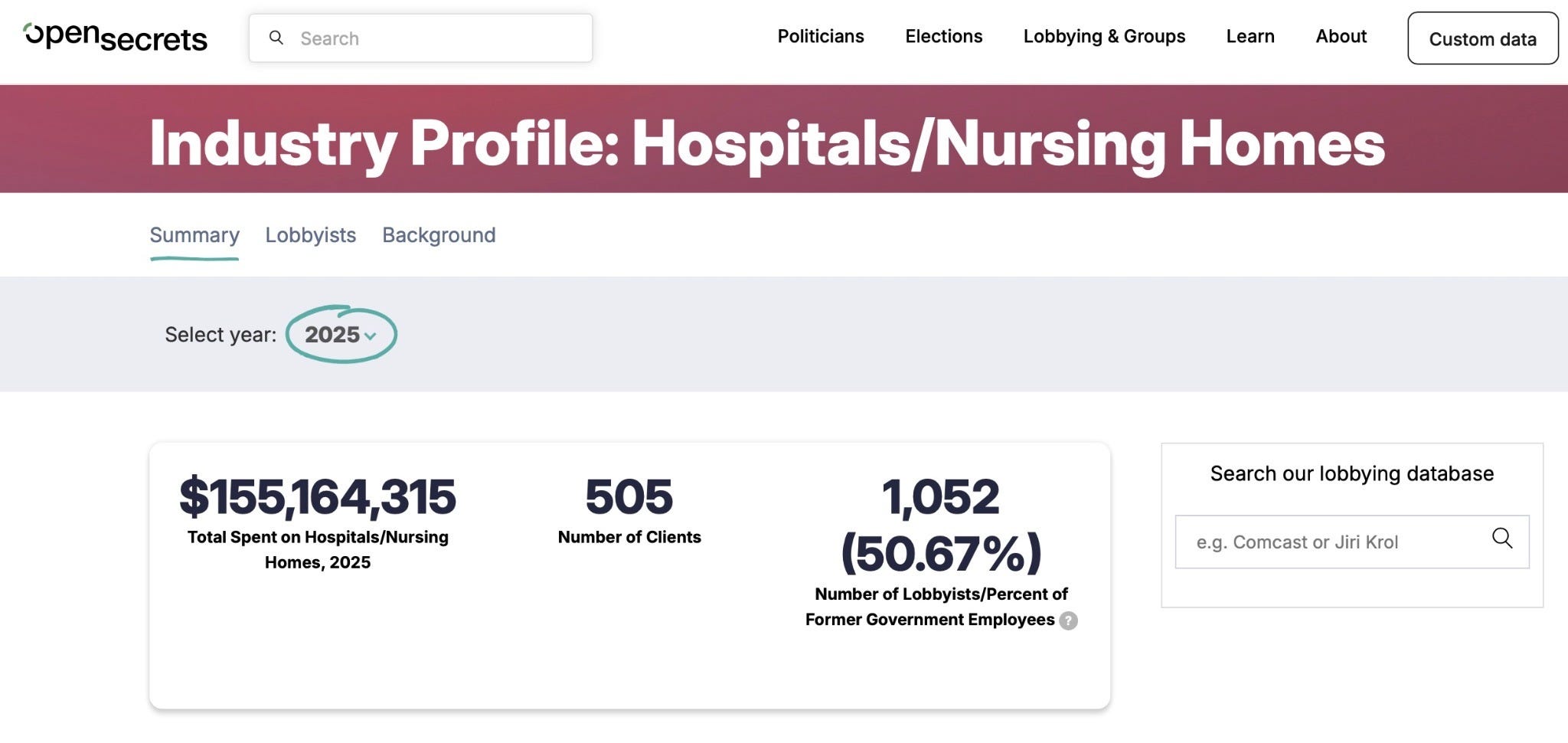
And of course, they lobby at industrial scale to smother any reform of these abuses, before it reaches a floor vote.
Despite this parade of horribles, sometimes (regrettably) you may actually need one.
What Hospitals Are Actually For
The system does have real, if narrow, uses. For a hospital proper, that use case is life-threatening emergencies.
I have a bullet in my belly.
I have a bone sticking out.
I’m having a stroke.
I’m having a heart attack.
I’ve drowned and I’m unconscious and not breathing.
My placenta is blocking the birth canal during delivery.
I have a tumor blocking my colon.
As I’ve written before, these are exactly the services that aren’t profitable for a hospital, and can’t be made profitable:
“The life-saving, acute services that are valuable are not profitable. They cannot be made profitable. They require an expensive crew of high-skill labor, cutting edge technology, the most expensive forms of ground and air transport, with 24/7/365 access for a catchment area that does not produce enough of these needs each year to recoup costs.” from Hospitals are Soviet-Style Hellscapes Unfit for Humans
The Stuff That Actually Pays the Bills
The rest of the hospital enterprise - the part that really rakes in the money - isn’t curing or healing much of anything. It’s suppressing symptoms, slowing disease progression, or preventing some hypothetical worse outcome that hasn’t happened and might never have happened.
Think:
Joint replacements
Chemotherapy and radiation
Mastectomies for breast cancer
So-called transgender procedures
Dialysis for advanced diabetes and kidney failure
Cardiac cath lab procedures - stents, balloons, and the like
Infusions for rheumatoid arthritis and other autoimmune disease
The majority of C-sections - as I’ve written before, for every genuinely emergent C-section, there are roughly two more elective or unnecessary versions, scheduled around a clock and a convenience, not a crisis
Very little of what actually generates revenue in a hospital is aimed at healing, curing, or reversing anything.
Plenty of the surgeries on that list have been shown in rigorous trials to perform no better than a well-run placebo. Some cancers resolve on their own or in spite of the treatment thrown at them - though it’s genuinely hard to pin an exact number on that, because we almost never test what would happen with radical lifestyle change or emotional healing tried alongside (or instead of) the poison-cut-burn protocol. Nobody’s funding that trial.
None of this means these treatments are all garbage, or that nobody needs them. Once you’re standing in the clinical presentation these procedures exist to address, the window for other options may already be closed. I’m not telling you to skip your chemo or your hip replacement.
What I am telling you is this: not one of us wants to be the person needing this care. Every single one of us would infinitely prefer never to need it at all. That’s the whole premium proposition of health - not needing to ever darken the door of these institutions.
All of these treatments represent the failure of health care, not health care itself. They are sick care. Sick care is what happens after health care has already failed.
Should Hospitals Even Exist As We Know Them?
I’m honestly not convinced hospitals should exist as financially independent entities at all. As we just covered, the services that actually save lives can’t be made profitable without the kind of cravenly corrupt cross-subsidizing we just walked through.
Maybe hospitals should simply be allowed to be what they actually are: the known money-losing wing of a larger operation that profits when people stay healthy. Some employers have already started thinking exactly this way - floating the idea of building their own hospitals, designed from day one to lose money on emergency and trauma care, while the real value gets delivered through advanced primary care and world-class specialty care outside the hospital, in innovative, often physician-owned models.
Which brings us to the actual playbook.
If You Need a Hospital, Don’t Go to a Hospital
Ok, to be fair, if it’s a true emergency, go to the nearest ER, full stop, no footnotes. (PS if it’s a broken bone that’s not sticking out of the skin, try an ortho urgent care instead).
But if it’s not an emergency and you still need or want conventional medicine, the single most important decision you’ll make is this: don’t do it at your local hospital system, or at any facility with their logo on the door.
Hospitals have swallowed so many independent physician practices, imaging centers, labs, and surgery centers that finding the survivors takes a little effort. But they’re out there, they’re often physician-owned, and physician-owned facilities consistently post better outcomes than the hospital-owned version of the same service. Here’s the rundown, category by category.

Surgery
Outpatient, freestanding surgery centers exist for nearly every elective (the kind you schedule) procedure now - GI surgery, joint replacement, even a lot of cancer surgery. These are called ambulatory surgery centers, which is just fancy talk for a place you walk into in the morning and leave before dark. Some also keep a handful of overnight beds for more complex cases.
It is rare, at this point, for surgery to genuinely require a hospital-owned facility. A huge share of it is now done laparoscopically or robotically rather than the old rip-you-open approach.
Google “independent, not owned by hospital, surgery center in [your area].”
For orthopedic procedures specifically, ask AI: “is there an Ortho Forum affiliate near [your area]?”
If you’ve already found an independent orthopedic practice for your consult (which you should - steer clear of the ones with a hospital logo on their website), just ask your orthopedist where the independent surgery center is that he personally uses.
If your surgeon happens to be hospital-employed, he’s going to schedule you at the hospital, and when you push back, he’ll walk you through all the reasons your particular risk profile is so special that, unlike normal patients, you can’t be operated on outside the hospital. Get a second opinion from a truly independent surgeon. That explanation is, more often than not, garbage.
If you want help finding the cash-pay option, a vendor like MDSave lets you shop surgeries, procedures, MRIs, and infusions for a transparent price. Use it to pay cash and submit to your plan afterward if you’d like - or just use it to find where the independent options near you actually are, then book there through your normal insurance if you’d rather not self-pay.
Infusions
Freestanding infusion centers are excellent for chemo and other infused drugs - like the ones treating rheumatoid arthritis, psoriasis, and other autoimmune conditions. They almost always take your insurance. Find one near you through the National Infusion Center Association locator.
Even better than a freestanding center: ask your health plan whether they’ll cover home infusion. It’s often dramatically cheaper and more convenient for a plan to send a nurse and the drug to your living room than to pay hospital or community oncology clinic rates. Search for a provider through the trade association’s directory.

So the pecking order is: home infusion first, freestanding infusion center second, and community oncology practice as your fallback if neither of the first two is available. Community oncology practices still tend to overcharge for the drug and its administration - but at least you’re not also paying hospital facility fees on top of it.
Imaging
MRI, CT, ultrasound, mammogram, DEXA scan, x-ray - whatever it is, stay away from a hospital system for it. Find a freestanding radiology facility instead. They’re usually named something like “[Your Town] Radiology,” or just ask AI to find the independent imaging center nearest you.
These places almost always take your insurance, and their cash price frequently beats whatever your plan is actually paying on your behalf. So if you’re still working through your deductible, don’t lead with your insurance card - say you’re self-pay, pay the cash rate, and submit the receipt to your plan afterward for deductible credit.
I also like RadiologyAssist.com for booking a cash-pay appointment at an independent facility near you - or just use it to identify where they’d send you, then book that same location through your insurance if you’d rather not pay cash upfront.
And if you do end up in a hospital and get hit with the bill you knew was coming, don’t just pay it. Go pull out my free playbook for outsmarting the medical billing trap and use every page of it.
We close our series with a review: the way to sustainably lower health care costs in this country isn’t a financing trick, a new middleman, or a better contract - those are all important whack-a-mole tricks staying one step ahead of the bad guys. The real solution is needing less health care - especially the kind that is bankrupting the U.S. and eating up almost half of every federal dollar.
That starts with living like a human, so fewer problems show up at all. When something’s wrong but it’s not an emergency - consider a partner in healing outside the white-coat paradigm. And when you truly need conventional care, get it anywhere except the Soviet-style hellscape on the tax-free real estate down the street, profiting from lifelong patients while pretending to be a charity.
Nobody in Washington is coming to fix this for you. The real revolution is what you do the next time a scheduler tells you where you “have” to go.