

Operation Warp Speed 2.0 Is Happening. Right Now. While You’re Reading This.
Brought to you, as always, by Pfizer.

Right now - as in, this very moment - a group of economists and pharma-friendly policy types are sitting down to lunch, bankrolled by Pfizer (I was told privately), in Washington, D.C. to discuss a draft Executive Order (EO) that would hand the pharmaceutical industry everything it has ever wanted and then some.
I was invited to this lunch.
I sent my deepest regrets. I’m writing this instead.
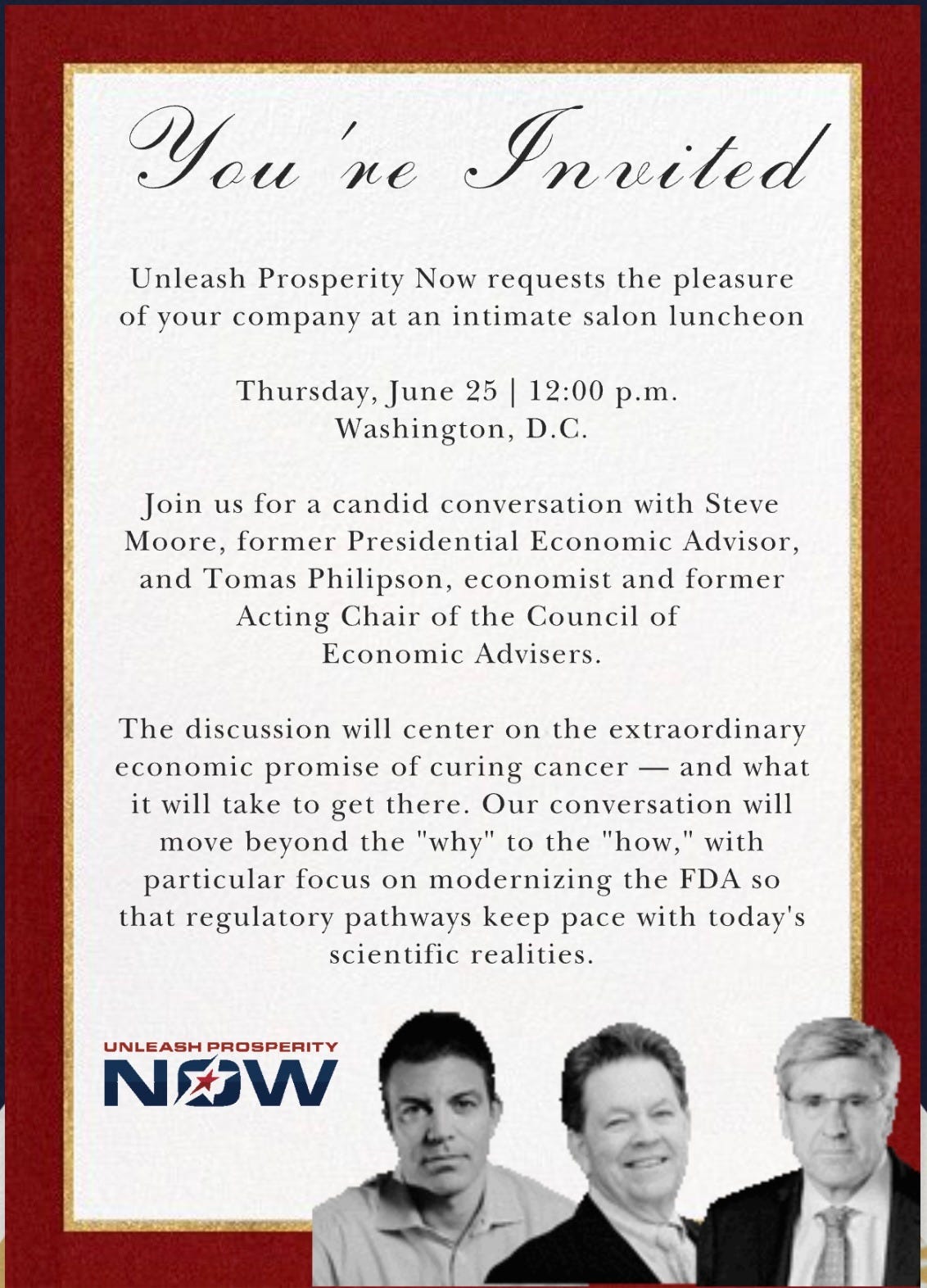
The event is hosted by Unleash Prosperity Now, the think tank founded by Steve Forbes. The featured guests are Steve Moore (former presidential economic advisor) and Tomas Philipson (former Acting Chair of the Council of Economic Advisors, and apparently the academic health economist behind this draft EO).
Now you might be wondering why any of us should care what a roomful of think-tankers, Pharma bros and ex-Trump advisors say to each other over lunch on Pfizer’s dime.
The very real concern is that these aren’t cranks shouting into the void. The powerful people who show up in rooms like this are serious players with strong ties to senior officials at the White House, at HHS, and the president himself.
And those ties aren’t just hypothetical. A draft cooked up by outsiders becomes real policy when someone on the inside thinks it has merit, picks it up and runs with it. One day it’s being passed around a salon luncheon. The next, it’s got the president’s signature on it.
I know, because I have my own version of that story. It’s how price transparency came to be. Pointing out this method isn’t a knock on anyone. It’s how good policy gets made, too. The difference is what’s getting pushed. That one was a populist issue, despised by industry interests, that polled at 90 percent with voters. This one is a wish list for Big Pharma and Well-Connected Biotech. Paid for by Pfizer.
It’s billed as “an intimate salon luncheon” to discuss “the extraordinary economic promise of curing cancer” and “modernizing the FDA so that regulatory pathways keep pace with today’s scientific realities.” Who could be against curing cancer or keeping up with science? I know this language.
I’ve spoken this language. I know the free-marketeering policy that it is code for - which I very often have agreed with over the past couple decades in conservative policymaking. But the Shakespearean flaw of laissez-faire economics is its knee-jerk defense of private industry interests in health care - even when, as in the case of the past decade or so, that industry has become increasingly indefensible.
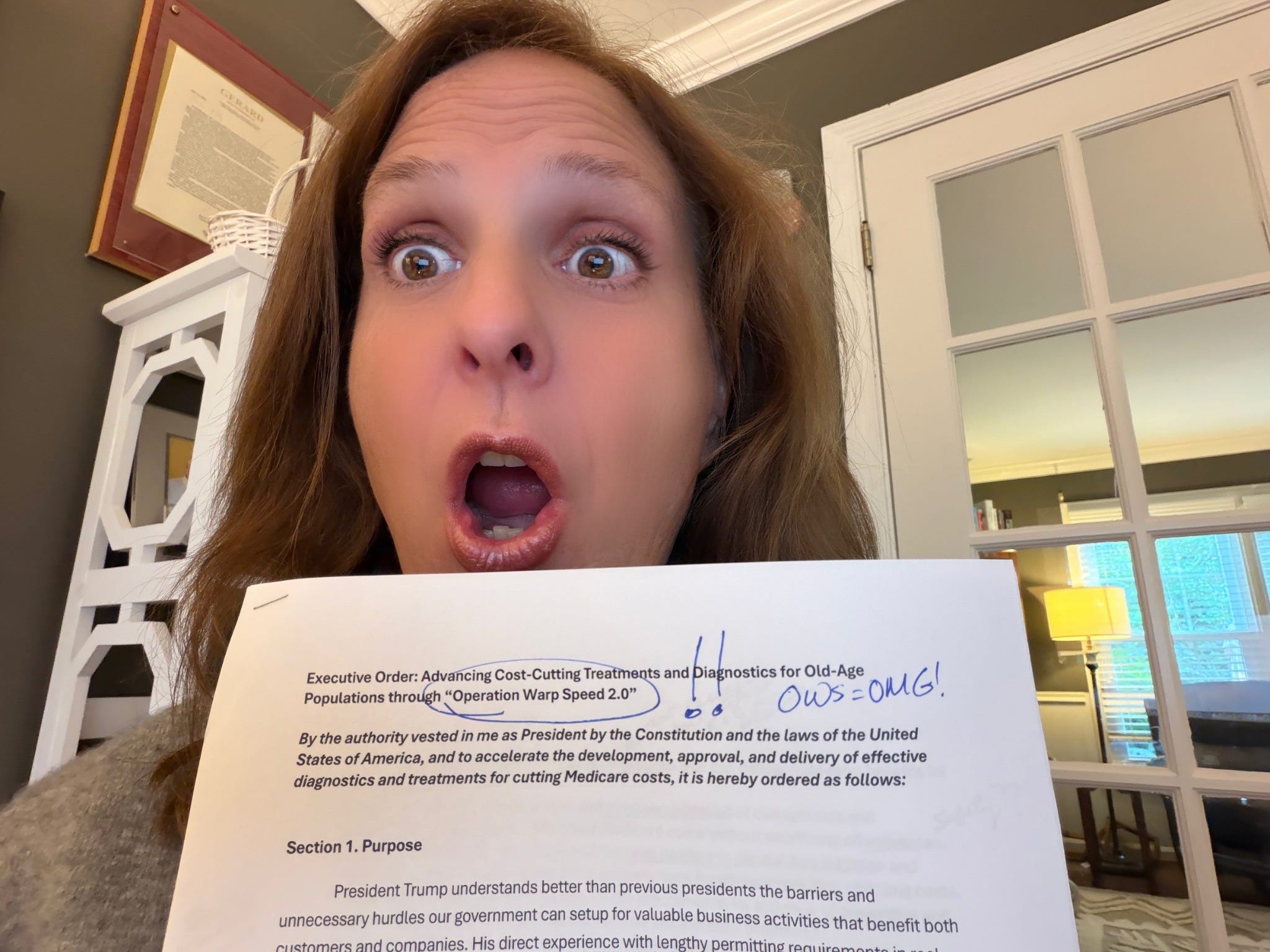
So I read what’s actually being proposed. Then I read it again, because I couldn’t believe my eyes.
And then I wrote 34 ranting comments in the margins.
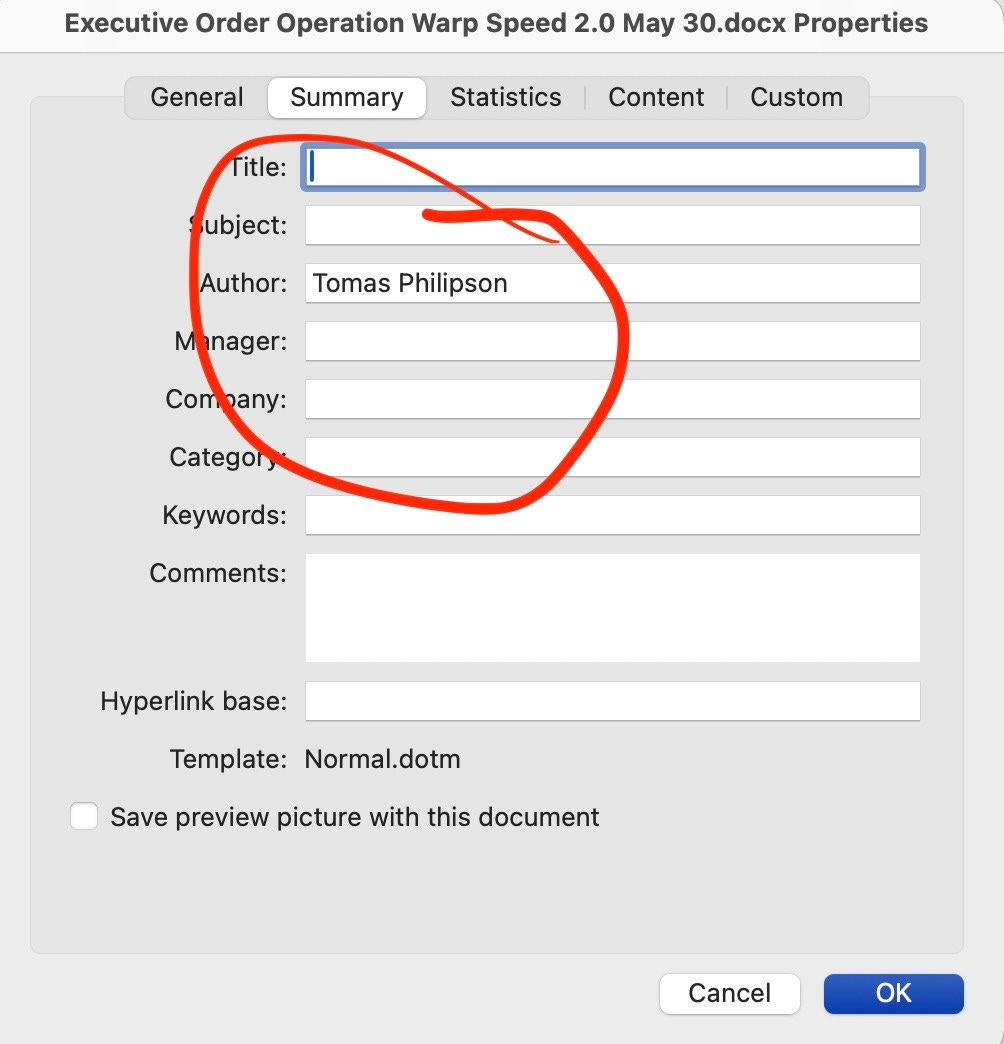
The metadata of the draft EO lists Tomas as its author, which of course doesn’t mean he doesn’t have other collaborators. I worked alongside Tomas in the first Trump White House. He’s committed, credentialed, and about as laissez-faire as they come - a University of Chicago health economist who made his bones arguing for policies just like those in the draft EO - less and less FDA as the key to more and more Pharma products.
The draft EO was attached to the invitation to this lunch as the actual subject matter to be discussed. It has a name: Advancing Cost-Cutting Treatments and Diagnostics for Old-Age Populations through “Operation Warp Speed 2.0.”
(Paid subscribers can read it for yourselves here.)
Where to Even Begin
Before we get into the substance, the name alone will doom this proposal with public opinion.
The president gets booed at his own rallies, by his most diehard supporters, when he brings up Operation Warp Speed. There is no constituency in the United States - not Republican, not Democrat, not MAHA, not libertarian, not the guy who got the shot or the guy who didn’t - who is enthusiastic about resurrecting that program. Operation Warp Speed and all it delivered to the world is one of the most politically radioactive policy episodes of the last decade, and whoever suggested that branding either doesn’t read the news or wants the president’s polling to crater.
But the name is obviously just the first of many tone-deaf self-owns in this document. Let’s go section by section.
The Founding Myth
The EO’s opening premise is that medical innovation is the key to controlling the federal debt. If we just cure cancer and Alzheimer’s, the argument goes, we won’t have to cut Medicare - we’ll have a healthier population that doesn’t need as much of it.
This sounds good. And if we actually cured Alzheimer’s, cancer, and the other diseases consuming Medicare’s budget, it would be true. But pharmaceutical innovation and disease elimination are not the same thing.
We have had unfathomable medical innovation over the past century. More drugs, more devices, more diagnostics, more interventions than any previous civilization could have imagined. And what do we have to show for it on a population level? We are chronically sicker, fatter, more mentally ill, and more infertile than any previous generation in human history. The extinction-level chronic disease crisis that is actually bankrupting Medicare is not a failure of pharmaceutical innovation. It is the predictable outcome of dehumanized, unbiological lives - of industrial poisons masquerading as food, sedentary routines disconnected from nature, epidemic sleep deprivation, chemical exposures, and severed social bonds.
Medical innovation is not the answer to these problems. It is, at best, an increasingly expensive way to manage their consequences while the causes go unaddressed. Even if you concede that some drugs are keeping people with significant disease alive a little longer - which may be true - that would only perversely drive costs up, as these expensive new therapies generally manage or extend decline during the most expensive end-of-life years, but don’t cure.
And the dirty little secret is that “innovation” has become the industry’s word for obscene launch prices.
When a drug company insists that a new therapy deserves a $400,000 annual price tag, they justify it by saying - there was R&D involved, there were trials, there was a regulatory process. What they are not telling you is how much of that R&D was publicly funded, how taxpayers will be footing the bill for these products used by Medicare beneficiaries, and yet, how completely the profit is privatized once the product hits the market.
If the past is any preview of the future, there is no universe in which this dynamic controls the federal debt. It accelerates it.

The EO describes Operation Warp Speed (v.1.0) as an inspiration. I’d like to offer some alternative framings:
The tens of thousands of deaths attributed to the vaccines. The epidemic of myocarditis in young people. More than a million adverse events reported to government surveillance systems called V-safe and VAERS. The Pfizer trial in which there were more deaths in the vaccinated group than the unvaccinated group - and we approved the product anyway, because Warp Speed. The systematic delegitimization of existing treatments that might have helped people but were made of molecules too old to be profitable.
I’m not interested in re-litigating the entire COVID response here (though you can read more of my thoughts on it elsewhere). But if the lesson your team drew from that experience is “let’s do that again, but for cancer,” you’ve spent too much time in the faculty lounge.
The Structure - Who’s Running This Thing?
The EO would establish an Operation Warp Speed (OWS) 2.0 Steering Committee to be headed by Secretary Kennedy and his key agency heads.
Secretary Kennedy.
You know, Robert F. Kennedy, Jr.
Who literally wrote a book trashing OWS 1.0.
The Steering Committee gets better. It also explicitly includes pharmaceutical and biotechnology companies, among others, who would direct and oversee the OWS activities.
In other words, the regulated entities would sit on the committee telling the regulators what to do.
This isn’t a new idea. It is, in fact, the defining feature of regulatory capture - the thing that RFK Jr. has spent decades fighting, the thing that MAHA exists to dismantle, the thing that former Commissioner Marty Makary named as a foundational problem when he walked into the FDA, long before he was shown the door.
And the dirty little secret is that “innovation” has become the industry’s word for obscene launch prices.
The EO summons another agency to the Steering Committee: BARDA, aka the Biomedical Advanced Research and Development Authority. You know, the shadowy, Pentagon-adjacent slush fund dressed up in public health clothing where sole-source contracts, guaranteed taxpayer pre-payment for unproven technologies, and relationships of unusual coziness with favored companies have determined who gets billions and who doesn’t.
What could possibly go wrong?
But the Operation Warp Speed (OWS) 2.0 Steering Committee isn’t the only committee this EO would establish.
The New “Advisory Committee on Expanding the FDA Mandate Beyond All Recognition”
Ok, that’s not really the name.
The EO would also create a permanent FDA Advisory Committee on Economic Innovation and Impact - a body of health economists, regulatory experts, industry representatives, biomedical entrepreneurs, and (for cover) patient advocates. The committee would be tasked with evaluating the economic consequences of FDA regulatory decisions and would require the FDA to respond in writing to any finding it declines to adopt.
Let me translate this: instead of asking whether a drug meets the scientific standard for approval, FDA would be pressured to ask whether enforcing that standard might hurt the industry’s (or anyone else’s) economic interests.
FDA’s statutory mandate from Congress is to protect the public from dangerous and ineffective products. Full stop. It is not to goose the GDP or pom-pom American biomedical competitiveness. It is not to weigh the complex economic ripple effects of its safety determinations. It is not to answer to industry representatives who are unhappy that their products didn’t get approved fast enough or that their garbage data were uncompelling.
The idea that an agency entirely organized around making scientific determinations about medical products has the institutional competence to accurately model all the downstream economic consequences of its licensure decisions is, charitably, delusional. No government agency could pull off such a sweeping set of mandates. And more to the point: we shouldn’t want it to try.
Picture the committee - stacked with regulated companies and their pals, now empowered to demand that their regulators consider the economic harm to their companies as part of the drug approval process. FDA’s independence has been in question for quite a while - in the last year, it’s been on life support. This would render it a complete fiction.
The draft EO reassures us that the committee members would be subject to “standard federal conflict-of-interest disclosure requirements.” But this is a joke - the committee is conflicted by design. The purpose of putting industry on the committee is to have industry’s interest overtly represented and to bully the FDA scientists with it.
FDA’s independence has been in question for quite a while - in the last year, it’s been on life support. This would render it a complete fiction.
Also worth imagining: this committee gets inherited by a future administration with completely different politics. Imagine President AOC, who decides that a drug’s anticipated launch price is itself grounds for withholding licensure. Because, economic impact. You’ve just built them the playbook - congratulations.
The Regulatory “Modernization” (Read: Weak-sauce Safety Trials)
Under the advice and oversight of all these committees, the draft EO would require:
Creating fast-track pathways that cut development and approval costs by at least 50% while “maintaining standards of safety and efficacy.” You can’t cut the cost and time of safety evaluation by half and then claim you haven’t touched the standards. Sufficient follow-up time to detect safety signals IS the standard.
Approving drugs that show “favorable safety with limited efficacy data” and then “further confirm safety and efficacy” later, by collecting more data after approval. But of course, shorter timelines make it less likely that we’ll know anything at all about safety, not more. This is the same trade the industry always wants: weaken and shorten pre-licensure requirements in exchange for post-licensure promises. Once a drug is on the market and a manufacturer blows off its post-market obligations, FDA is quite hamstrung in terms of what it can do without incurring the wrath of lawsuits and patient revolt. I don’t want to have to “further confirm” safety after licensure. I want safety fully confirmed before licensure. That used to be the whole point.
FDA’s statutory mandate from Congress is to protect the public from dangerous and ineffective products. Full stop. It is not to goose the GDP or pom-pom American biomedical competitiveness.
Establishing a quota: prioritize approval of at least three breakthrough therapeutics by June 2028. This is not how regulatory science is supposed to work. If products meet the statutory standard, they get approved. If they don’t, they don’t. Setting an approval quota in advance is just explicit pressure on regulators to cut corners to meet the number. If you don’t believe me, ask Drs. Marty Makary, Vinay Prasad, Tracy Beth Høeg, and every other FDA scientist who has faced industry pressure to lower their standards.
Streamlining biomarker validation and surrogate endpoints for drug approvals. In other words, use change in some lab result as the outcome studied in the trial instead of, you know, actual improvement in health or mortality. I will be generous here: there are some biomarkers that are genuinely well-validated and useful as surrogate outcomes. But the track record on aggressive use of surrogates to speed approvals is not inspiring. Too many drugs approved this way improved the surrogate but were later discovered to have no impact on the clinical outcome (or to make it worse). Oncology drugs approved on progression-free survival that never demonstrated improved overall survival. The Aduhelm debacle for Alzheimer’s. The emerging scientific consensus - supported by decades of hard experience - is moving toward more rigor on surrogate validation, not less. This EO proposes to move in the opposite direction, and it does so, not because the science supports it, but because it lowers costs for drug makers.
Taxpayers as Insurance Policy and Piggy Bank
The EO directs NIH, BARDA, and the VA to use their contracting authority to “support late-stage trials and secure early access to promising candidates.”
If you don’t speak pharma gibberish, that means: transfer the financial risk of pharmaceutical R&D from private companies - who will capture all the profit - onto taxpayers, who will capture none of it. The companies bear the upside. The American public bears the downside. These frameworks have historically generated sole-source contracts, sweetheart deals for politically favored manufacturers, and guaranteed government pre-payment for unproven products.
As with so much else in this EO, we need less of this type of corruption, not more.
The Coverage Mandate
Buried in the coverage provisions is this: “CMS shall ensure that Medicare beneficiaries can access OWS 2.0-designated products within 30 days of FDA authorization.”
A drug gets FDA authorization under the accelerated approval pathway - meaning it has shown “favorable” safety (whatever that means) with limited efficacy data, remember - and within 30 days, Medicare must cover it. Before the “evidence development phase” tells us whether it actually works or has been followed long enough to be deemed safe.
This is guaranteed procurement by one of the planet’s largest single-payer systems, for under-scrutinized products at obscene launch prices, backed by the full faith and credit of the United States Treasury, with a 30-day clock that ensures there’s no time or leverage for the government to ask the hard questions or negotiate reasonable terms and conditions.
I’m old enough to remember when Republicans - especially Republican economists - argued that coverage mandates drive up the cost of health care.
And… Brace Yourself
Attention, MAHA: the draft EO calls for “ a rolling review process with clear timelines… similar to the Emergency Use Authorization (EUA) framework.”
I admit, I froze in horror and wrote “OMG” in the margins before I calmed down and read this part more carefully. Charitably, I think the EUA reference is really just about how the reviews of potential new products are scheduled (on a rolling basis to make the process more real-time and supposedly more efficient). I don’t think the EO is intending to use the EUA reference as a dog-whistle for a liability protection racket for industry here. But talk about tone-deaf! Between the OWS branding and the EUA shout-out, my MAHA moms are going to be calling their homeopaths for an acute PTSD remedy.
A Word for Our Friends Inside the Administration
I’m told that some people from HHS attended this Pfizer lunch. I hope it’s not true, or if it is true, that they’re using it as an opportunity to laugh this draft EO out of the room.
I have to believe that the few MAHA faithful who remain in the administration after the industry-instigated purge of the past year - Secretary Kennedy, NIH and CDC Director Jay Bhattacharya, and White House health advisor Calley Means - have not seen this document. These are people who have staked their careers and reputations on the proposition that the pharmaceutical-regulatory complex has been captured, that safety standards have been compromised by industry pressure, that the government has been de-risking pharma’s business model on the public’s dime, and that we need to fight all of that with everything we have.
This executive order is the enemy they’ve been fighting. It’s what they came to Washington to stop.
You can’t simultaneously lead a Make America Healthy Again movement and then go sign an executive order that puts pharmaceutical companies in charge of a new Operation Warp Speed designed to weaken safety and efficacy standards, mandate Medicare coverage of under-scrutinized drugs, and claim it’s all in the service of “lower costs” (LOL).
Those things can ‘t coexist, and the political base that elected this president knows it.
The Actual Answer
The draft EO closes with gestures toward lifestyle modification and AI tools for “personalized preventive guidance.”
It’s an afterthought.
The industry interests at the “intimate salon luncheon” going on right now will likely deflect attention from the four leading risk factors for preventable chronic disease - garbage food, physical inactivity, tobacco use, and excessive booze. These account for more than half of all preventable disease deaths in the United States across cancer, cardiovascular disease, chronic respiratory disease, and diabetes combined.
Folks, none of us suffers from an inborn pharmaceutical deficiency. What we suffer from is: not living like humans, for the past few generations.
Addressing these factors is hard. Much harder than turning a blind eye to unconvincing trial data and slapping an approval stamp on Pharma’s latest blockbuster. It requires taking on the food industry, the chemical industry, the seed oil lobby, the pharmaceutical companies that profit from managing the consequences of these diseases instead of preventing them. It requires telling Americans stuff that none of us wants to hear (You’re fat! Get off Diet Coke!). It requires regulators committed to protecting the public from misaligned industry interests rather than protecting industry from the public - public scrutiny, accountability and legal liability.
The cheapest disease to treat is the one that never develops in the first place. The biggest ROI is in prevention and lifestyle-mediated disease reversal, not weak-sauce symptom mitigation to manage and extend decline.
Nobody’s fooled by the pretense that this draft EO is about lowering costs for seniors and taxpayers. Throwing billions more at Pharma and transferring the R&D risk of drug development from them to us lowers nobody’s costs but Pharma’s.
The truth is that this policy is just craven regulatory capture and we have to make sure it never makes contact with the business end of President Trump’s pen.

I would say I'm shocked, but then I remember when they played Pandemic prior to Covid. Pretend play in the DMV often ends up becoming headlines in real life. Either let FDA actually regulate or shut it down and let pharma sell what they want honestly - without a fake "safe and effective" stamp used to deceive patients. I'm personally not interested in funding drugs that hurt people.
Surrogate markers are such a big one. I recently started looking into the supposed evidence that everyone needs more fiber, and I found:
1. It increases the variety of beneficial bacteria in your stools. [I think this is my favorite surrogate marker ever]
2. It eases constipation. [Well, not everyone is constipated].
I'm not convinced.
Great piece as usual, Katy.